

After informed consent and necessary pre-op preparation patient is taken to operation theatre and given general anaesthesia.
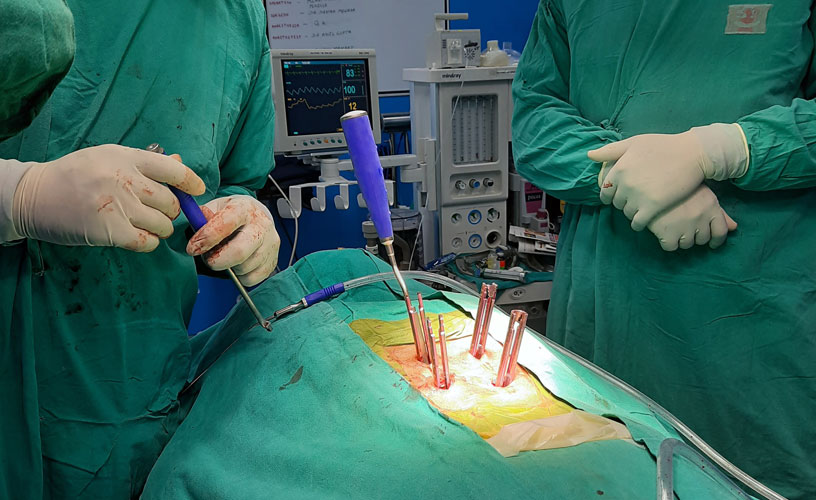
Spinal decompression is then done followed by spinal fixation using Titanium implants (screws, rods and/or plates). Bone grafts are used for spinal fusion wherever applicable for good results.
Patient is usually shifted to ward and is made to stand / mobilised from the next day. Physiotherapy and rehabilitation is further monitored by experienced team of physiotherapists along with the surgeon.
In most cases there is significant improvement in terms of pain relief and neurological recovery with rare incidence of failed surgery / neurological deterioration with present surgical techniques and advanced instruments.
Surgery for Pott’s Spine
- C7-D2 collapse with C3-D5 pre & paravertebral collection with spaticquadriparesis - Pott’s Spine
- C7-D2 laminectomy & decompression with drainage of abscess with C5C6-D3D4 fixation
Craniovertebral Junction (CVJ) Stabilisation Procedure
- Post-traumatic C2 Fracture with AAD with Quadriparesis & BBI
- C1 (lateral mass screws) – C2 (pedicle screws) Fixation using C1 reduction screws
Excision of Spinal Tumor
- Lumbar Spinal Tumor (expansile lytic lesion) with paraparesis & BBI
- Complete excision of tumor with spinal fixation and stabilisation
Spinal Decompression and Fixation for Spine Injury
- D12# with cord compression & contusion with paraplegia & BBI
- D12 partial corpectomy& decompression with D11-L1 pedicle screw fixation & fusion using expandable interbody cage filled with autologous bone graft


